


For Whom Has the Pandemic Ended?
The ongoing pandemic in America's most impoverished counties.

Summary: When President Trump pushed back on pandemic mitigation in April 2020, 100,000-240,000 deaths were expected from COVID-19. As President Biden and Congress declare the pandemic “over” this same rate of per capita mortality sits in our most impoverished counties. Yet few are speaking up.
“The pandemic is over.”
United States President Joe Biden spoke these words on Sunday, September 18, 2022 as he strolled through the Detroit Auto Show while being interviewed for 60 Minutes. Many were pleased to hear these assuring words. Normal life must be around the corner - and for many who had ignored the reality of the pandemic for months, normal behavior had already returned.
Yet other people were aghast. In the week prior to President Biden’s interview, 2,800 people in the United States died from COVID-19. 2,700 more would die during the following week. Infections remained high and far too many continued to suffer from the debilitation of long-covid. For these people, confusion and disbelief rang through the President’s words.
When we look at the setting of the interview, we begin to understand the President’s intent more clearly. He spoke from middle America. On full display behind him sat the products of the America’s most iconic industry - automobiles. The view gave us a hint as to his intended audience. He directed his message to affluent and middle-class America as well as to corporate leaders. These were the people whose votes he needed in the upcoming November 2022 mid-term election. His statement was not addressed to those suffering the most from the pandemic.
Throughout the pandemic there have been large discrepancies in health outcomes. People of color have suffered higher rates of morbidity and mortality than white people. The difference is even more striking when compared to the population of college educated white people. Examining rates of COVID-19 mortality during the year 2020 Justin Feldman and Mary Bassett found that there would have been “71% fewer deaths among racial and ethnic minority populations” had these populations experienced the same rate of COVID-19 mortality as the college educated white population. Even in the more recent months of the pandemic, when some pundits lauded the success of lessening racial and ethnic divides in pandemic outcomes, the real discrepancies continued. For instance, during the height of the omicron wave, Dielle J. Lundberg, Elizabeth Wrigley-Field, and colleagues found that the majority of the decrease in disparities between deaths in the Black and white populations occurred due to "increases in mortality among non-Hispanic White adults and shifts in mortality to nonmetropolitan areas, where more non-Hispanic White adults reside.” After centering its most severe devastation on the east and west coasts, the pandemic invaded the heartland during the summer of 2020. In particular, the pandemic invaded areas of the interior suffering from poverty. The decreased racial and ethnic disparities that some noted didn’t occur because we became better at protecting racial and ethnic minority populations but instead because the pandemic took firmer root in economically vulnerable rural America.
The following two graphs display (Figure 1) the monthly deaths per million residents for the 10-percent of most and least impoverished counties since the pandemic began and (Figure 2) the ratio of deaths of the most to the least impoverished counties.

Figure 1. Average rate of COVID-19 deaths per one-million residents in counties that rank in the 10% of most and least impoverished counties. Data collected from USA Facts and the U.S. Census Bureau.

Figure 2. Ratio of average rate of COVID-19 deaths per one-million residents in counties that rank in the 10% of most to least impoverished counties. Data collected from USA Facts and the U.S. Census Bureau.
Throughout most months of the pandemic to date, deaths in the most impoverished counties have been two to three times larger than those in the least impoverished counties. In some months the difference has been over four times as large.
For reference, the high poverty counties have an average rate of poverty of 29-percent and the low poverty counties have an average rate of 7-percent. In the most impoverished counties, an average of 37-percent of children live in poverty. This difference in pandemic outcomes is not a result of differences in age. The least impoverished counties are marginally older (42 years of age to 38) than the most impoverished counties and each set of counties contains about 2-percent of residents who are 85 years of age or older. The least impoverished counties are overwhelmingly white (83-percent). These counties have scant Black (3-percent) and Native American (1-percent) populations. In contrast the most impoverished counties have Black (26%) and Native American (7%) populations much larger than national averages. There are fewer Latinx people in the least impoverished counties (8-percent to 12-percent) and slightly more Asian-Americans (2-percent to 1-percent). Where do these counties sit geographically? Rural America. They are concentrated in states like Alabama, Arkansas, Florida, Georgia, Kentucky, Louisiana, Mississippi, Missouri, New Mexico, North Carolina, South Carolina, South Dakota, Tennessee, Texas, and West Virginia.
Of course, poverty alone doesn’t directly create more pronounced harm from the pandemic. However, all of the things that exist side by side with poverty do. Start with healthcare. People living in the most impoverished counties hold fewer health care resources than those in the least impoverished by significant margins across any metric you choose. For instance, people in the most impoverished counties have higher percentages of people without health insurance (14-percent to 7-percent), fewer hospitals to treat patients, and fewer ICU beds available (13 ICU beds per county to 20). Further, 60-percent of the most impoverished counties have no ICU beds at all within the entire county. Not a single one! People in these locations must leave their county to be treated for the most severe cases of COVID-19.
Lack of high-quality healthcare prior to the pandemic led to other issues. Rates of diabetes and obesity are higher in the most impoverished counties by 70-percent and 26-percent. Many of these people live in food deserts where nutritious foods are unavailable or unaffordable. Our lack of care for people in poverty during normal times created a portion of the severe pandemic inequality for impoverished people and for people of color. Of course, there are other factors that created more exposure for more impoverished areas such as higher rates of overcrowded and multi-generational housing, higher frequency of public transportation use, and a greater representation in face-to-face jobs that more easily allow for transmission.
Going back to our fears at the beginning of the pandemic, on March 31, 2020 Donald Trump, Deborah Brix, and other members of the White House coronavirus task force met the American people with shocking news. Experts on the task force reported that we should expect 100,000-240,000 United States fatalities from the COVID-19 pandemic. At the time even 100,000 deaths seemed an astounding number. At the end of March 2020, we felt that we were in the thick of the pandemic and the total death count to sat at about 3,800. Could it really get worse? At the time, the death of 100,000-240,000 Americans from a pandemic in a world of modern science and medicine was unthinkable to most.
To many cynics 100,000-240,000 predicted deaths seemed to be the inverse of the classic adage to under-promise and over-deliver. If the Trump administration could keep U.S. deaths below these numbers he could claim a win – and we know how Donald loves to claim a win even in the face of defeat. Of course, history has provided the stark opposite of a win, by anyone’s definition. Yet we now know how understated the worst-case fears were and how badly we lost. When the pandemic began, no one expected over one-million parents, grandparents, sisters, brothers, cousins, partners, spouses, children, caregivers and other loved ones to die in the United States. Yet, here we are.
Three years later at the “end of the pandemic emergency” where do we sit for the people in most danger? In the following graph I display monthly COVID-19 death rates since May 2022, again for the most and least impoverished counties.
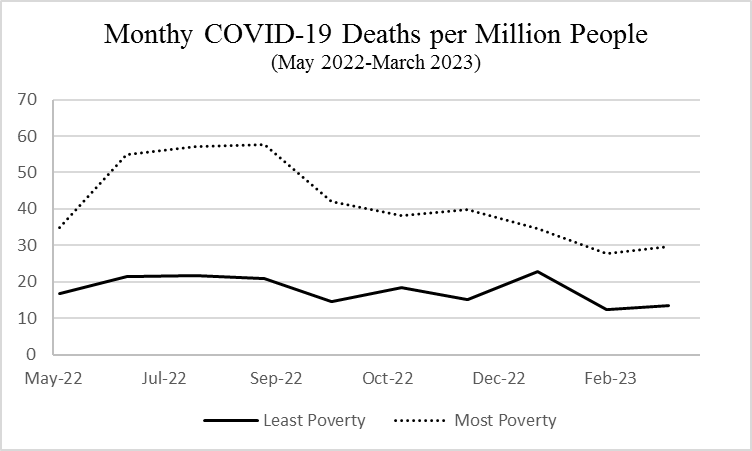
Figure 3. Average rate of COVID-19 deaths per one-million residents in counties that rank in the 10% of most and least impoverished counties. Data collected from USA Facts and the U.S. Census Bureau.
The discrepancy continues between areas impoverished and not. Over the past six months the most impoverished counties have faced an average rate of death from COVID-19 of about 35 deaths per million residents. If this rate of COVID-19 mortality extended to the entire United States population it would equate to about 11,600 deaths per month and 140,000 deaths per year. This amount of devastation matches our worst fears presented by the coronavirus task force in March 2020. The most impoverished areas of the country continue to live in these circumstances today. In spring 2020 this level of expected danger caused us to close schools and non-essential businesses, to implement wide scale social distancing measures and mass gathering limits, and required masking within indoor public spaces throughout the country. This 2020 reality of pandemic devastation is still being lived today among the most impoverished areas of the country. To be clear, these are not the only areas of the country and the only groups of people still affected by the pandemic. The pandemic continues to be a danger for everyone but the most danger lies with people who are economically vulnerable and those who are medically vulnerable for a variety of reasons. All of these people need to be protected from the pandemic that still haunts us. It is our responsibility as a society to protect everyone not just the most fortunate among us. We don’t need to return to the all of the mitigation measures of spring 2020. However, we can’t abandon these people. Yet, this is what many are doing.
Our leaders in Washington have stated that the pandemic emergency is over with fell swoops of presidential and congressional pens. Many of our leaders in state capitals, at the CDC, and at the WHO are now dismissing the pandemic danger too. It is a travesty to leave these people behind when we would never do so if this rate of pandemic morbidity and mortality was spread across the entire nation and particularly among the voters that politicians depend upon for their political and financial support. As Harvard epidemiologist Justin Feldman wrote over two years ago, “up to March 2021, there were fewer than 5,000 Covid deaths among college-educated white people under age 65 in the U.S., which is likely why it has been so easy for those in power to downplay the severity of the crisis.” When he wrote these words politicians were doing away with mask mandates. Now, they are doing away with concern for the pandemic altogether.
With the end to the pandemic national emergency last week, we are leaving our most vulnerable people to fend for themselves. They will soon need to pay for tests, vaccines, and treatments such as Paxlovid or other anti-viral drugs out of their own pockets. These fees alone may run into the hundreds or thousands of dollars for some families. Beyond these fees those with more severe illness will need to pay fees or insurance co-pays for physicians, urgent care visits, and hospital stays. Where is this money going to come from when many of the families most impacted by the pandemic struggle to attain food, clothing, and shelter even when not facing a pandemic?
President Biden, do not leave these communities and people behind. You can do better. These people deserve better. We all deserve better.
Troy Tassier is an economist at Fordham University in New York and the author of the forthcoming book, The Rich Flee and the Poor Take the Bus: How our unequal society fails us during outbreaks, available from Johns Hopkins University Press in 2024.